

Dr John Chaplin – Auckland Head and Neck Specialist
Resecting head and neck cancers, benign tumours and major trauma to the face and neck can create large defects that have a profound effect on cosmesis and function. Over the past 25 -30 years significant advances have been made in improving patients functional and aesthetic outcomes following creation of these defects. Most of the advances have been in reconstruction of the defects with autologous (the patients own) tissue. A number of important anatomical donor sites have been identified from where complex tissue can be removed with its own blood supply with minimal donor site problems. Some of these sites are near the head and neck so the tissue can be moved but is anchored by a pedicle (pedicled or regional flaps) and some are from distant sites. The tissue from these distant sites is brought up with an artery and vein that are then anastomosed (joined) to blood vessels in the neck to ensure a robust blood supply. This technology is called Free Tissue Transfer and the components are referred to as Free Flaps.
Soft Tissue Flaps
These can be local, regional or free flaps from distant sites. The choice of flap depends on the size , site and complexity of the defect that needs to be reconstructed. Ideally one would like to replace the tissue removed with exactly the same type of tissue. However this is frequently not possible and substitute tissue is used.
Local Flaps: tend to be used to reconstruct smaller skin defects in the face, scalp and neck that cannot be closed primarily or skin grafted. There are a variety of these based on the blood supply to the skin. They are limited by size and by the arc of rotation from the attachment.
Regional flaps: These flaps are based on a named artery and can be larger and consist of more than one type of tissue. eg The pectorlais major flap consists of muscle alone or muscle and skin. These flaps have long been used in head and neck reconstruction for a wide range of defects, they still play an important role but they are limited by their attachments and their uses are now better defined. The donor sites include: pectoralis major, latissimus dorsi, deltopectoral.
Free Flaps: Offer great versatility, better tissue match and unlimited range of rotation and reach. There are several donor sites that are used. The radial forearm is the most versatile and widely used. Others include: Ulnar forearm, Lateral arm, Scapular and Parascapular, Latissimus dorsi, Rectus abdominus, Anterolateral thigh, Gracilis, Tensor facscia lata. These flaps are very reliable and can be used to reconstruct complex, large and multicomponent defects.
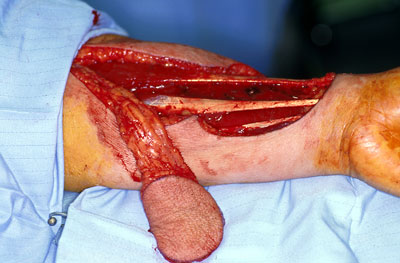 Left Radial Forearm Free Flap Elevated and in Situ.
Left Radial Forearm Free Flap Elevated and in Situ.
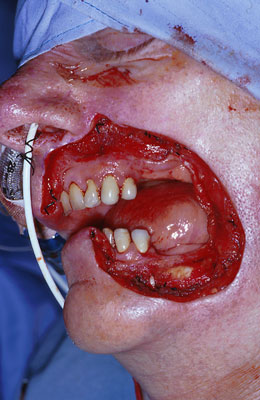
Forearm Free Flap Used to Reconstruct Left lateral Tongue Defect
Large Cheek Defect for Removal of Recurrent Cancer of the Lip and Reconstruction with Radial Forearm Free flap
Bone Containing Free Flaps
 Cancers of the head and neck, particularly in the oral cavity can involve bone of the upper and/or lower jaw. Frequently bone needs to be removed to adequately remove tumour and this can result in a defect that can have a marked impact on function. Free flaps containing bone are used to reconstruct these defects and restore form and function following ablative surgery. The most common bone free flap used is the fibula but iliac crest and scapula are also used in special situations.
Cancers of the head and neck, particularly in the oral cavity can involve bone of the upper and/or lower jaw. Frequently bone needs to be removed to adequately remove tumour and this can result in a defect that can have a marked impact on function. Free flaps containing bone are used to reconstruct these defects and restore form and function following ablative surgery. The most common bone free flap used is the fibula but iliac crest and scapula are also used in special situations.
Fibula free flap marked out on the leg. The skin elipse has perforating blood vessels that have been identified with a doppler marked on it.
The flap harvested and ready to inset into the defect.The late intra-oral

appearance of the skin paddle draped over the bone following fibula free flap reconstruction of a right lateral segmental mandibular defect for squamous carcinoma of the lower alveolus.


